

Introduction
Plasma cell-free DNA (cfDNA) and circulating tumor DNA (ctDNA) genotyping in Diffuse Large B-cell Lymphoma (DLBCL) holds great promise for early detection and response prediction. DLBCL is a highly heterogenous disease with diverse tumor behaviour and outcomes, yet the delineation of poor- risk groups remains challenging. Genomically driven molecular risk stratification, using ultradeep next generation sequencing (NGS) provides a comprehensive view of the mutational landscape of lymphoma and enables ultrasensitive disease detection.
Here, we present an interim analysis of ctDNA kinetics from ACCEPT, a phase Ib/II study of acalabrutinib with rituximab, cyclophosphamide, doxorubicin, vincristine and prednisolone (R-CHOP) for patients with previously untreated DLBCL.
Methods
Plasma samples were collected at four time points, at baseline and before the second, third and final cycles of chemotherapy. Extracted cell-free DNA (cfDNA) was quantified by fluorometry, prior to undergoing library preparation and next-generation sequencing using the CAncer Personalized Profiling by deep Sequencing (CAPP-Seq) methodology. The targeted sequencing panel covered 799 regions over 50 genes (>200Kb) known to be involved in lymphomagenesis. Analysis was carried out with a custom bioinformatics pipeline using error-corrected deduplication and a database of known artefacts to reduce background noise and improve sensitivity for low-level somatic variant detection. Patients were closely monitored through the study period by clinical examination and PET-CT scanning to provide objective endpoints against which the ctDNA response could be correlated.
Results
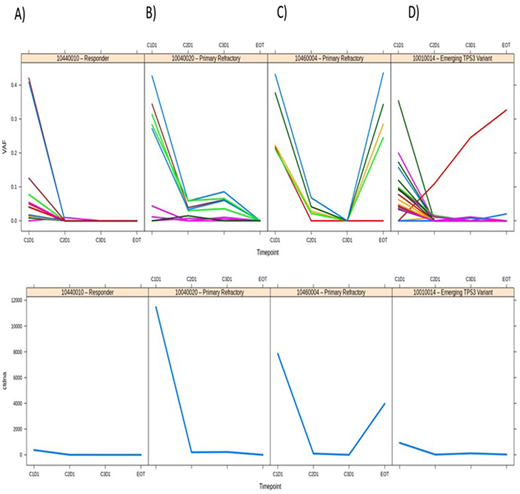
Fifteen patients had samples analysed for all four time points at the time of the interim analysis and were included in the study. Ten (66%) had late stage disease, nine (60%) poor risk disease (IPI > 2). Early vs late stage of disease at presentation showed a strong correlation with baseline levels of both total cfDNA (3,946 HGE/ml vs 21,613 HGE/ml) and ctDNA (842HGE/ml vs 6,380 HGE/ml). Twelve patients (80%) had trackable variants detected at baseline. The majority of these cleared after the first cycle of chemotherapy (Figure A; representative patient). Two cases (Figures B and C) had variants persistently detectable at high variant allele frequency (VAF) (0.059 and 0.068). These patients both had primary refractory disease. One patient from the first acalabrutinib dose escalation cohort and the second patient was found to be ineligible and withdrawn from the primary analysis because of continuous co-administration of omeprazole during therapy which inhibits acalabrutinib absorption. All others achieved a metabolic complete metabolic remission (mCR) after the final cycle of therapy. A third pattern of response noted was (Figure D) showing disappearance of detectable variants at baseline but progressive emergence of an acquired TP53 variant throughout follow-up that was not detected in the patient's germline sample. This high-risk patient with IPI of 5 and triple-hit DLBCL achieved a mCR and remains in remission in follow-up.
Conclusion
The clearance of ctDNA from the plasma of the responding patients in our study is consistent with the prior literature, as is the poor prognostic significance of persisting variants after the first cycle of chemotherapy. The rapid kinetics of the changes in ctDNA is noted and is potentially of advantage over other modalities of monitoring, such as PET-CT scan. Data on the entire cohort (n=30) and longer follow-up will be available at the time of the meeting.
Davies:Roche: Other: TRAVEL, ACCOMMODATIONS, EXPENSES; Roche, Celgene, Kite Pharma, Acerta, Karyopharma, Regeneron, Incyte: Consultancy; Roche, Acerta Pharma, AstraZeneca, Celgene, Gilead, ADC Therapeutics, Gilead: Research Funding; Celegene, Roche, Kite Pharma, Celegene: Honoraria. Johnson:Oncimmune: Consultancy; Bristol-Myers: Honoraria; Celgene: Honoraria; Genmab: Honoraria; Incyte: Honoraria; Kite Pharma: Honoraria; Kymera: Honoraria; MorphoSys: Honoraria; Novartis: Honoraria; Takeda: Honoraria; Boehringer Ingelheim: Consultancy; Epizyme: Consultancy, Research Funding; Janssen: Consultancy; Oncimmune: Consultancy; Epizyme: Consultancy, Research Funding; Janssen: Consultancy. Schuh:Illumina: Other: Consulting fees; Roche: Other: Consulting fees; Gilead: Other: Consulting fees; Abbvie: Other: Consulting fees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal